You must be logged in to record observations.
Short Description
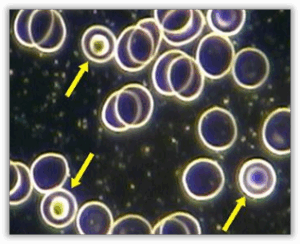
Target cells are red blood cells that display a distinctive bull’s-eye or target-like appearance, with a darker central area surrounded by a lighter ring and an outer rim. This pattern reflects an altered balance between the red blood cell’s internal content and its surrounding membrane.
In live blood analysis, it is not unusual to observe an occasional target-shaped red blood cell within a field of view. However, when a noticeable proportion of red blood cells show this characteristic appearance across multiple fields, it suggests a broader pattern rather than an isolated variation.
The presence of target cells indicates that red blood cell structure is being influenced by changes in membrane composition or internal distribution, highlighting a blood terrain where balance between cell content and surface area may be altered.
Appearance
The term “target cell” arises from the cell’s resemblance to a target. Also referred to as codocytes and anulocytes, these cells range from hypochromic cells, where the central area of pallor is much larger and more defined than usual, to true target cells that contain a bull’s-eye in the centre of the cell. This appearance is due to the RBC’s abnormal shape.
Pleomorphic Perspective
Target cells are erythrocytes that have become parasitised by the endobiont (Mucor racemosus Fresen). Dysbiosis is to be suspected whenever the shape or size of a blood form is disturbed. Codocytes are often observed along with “flimmering” (an acronym for flickering and glimmering, where the central area of the RBC seems to flicker or glimmer) in the RBCs, which indicates parasitism of the RBCs by microorganisms. This is a vegetative process where high-valence symprotits and ascits use a contained environment which provides nutritional reserves for their upward development. This infestation will become obvious in darkfield by pressing lightly on the cover slip with a pointed object like the tip of a pen, which will break up the RBCs and release the colloids from the cells. The advanced phases of the endobiont will often be found to be related to this appearance.
Medical Perspective
Hypochromia occurs when an erythrocyte contains a decreased amount of haemoglobin. It appears as a larger-than-normal central area of pallor with a thin rim of haemoglobin. This is one of the most commonly observed types of abnormal erythrocytes, seen in iron-deficiency anaemia and thalassaemia. It may also be seen in any haemoglobinopathy. Codocytes are erythrocytes that exhibit a dark circular ‘target’ pattern. They are seen in hypochromic anaemia, liver disease and occasionally after splenectomy. Erythrocytes with this configuration are cells lacking iron; therefore, any disease process that affects red cell iron absorption may produce target cells. Marked elevations of target cells can also result from a shift in the exchange equilibrium between red cells and cholesterol. Conditions that reduce lecithin-cholesterol acyltransferase production or interfere with enzyme mechanisms of performance result in elevated red cell cholesterol and serum phospholipid ratios. The bile salts content ratio in plasma can also affect cholesterol exchange between plasma and red cell membranes.
Relevance
Target cells can be present in the blood of healthy individuals, but usually comprise <1% of RBC population. The presence of more than 5 target cells in the sample would be considered a significant finding, especially if accompanied by the symptoms of anaemia. However, in a case where more than 10% of the RBCs are microcytic and hypochromic (and where some anaemia symptoms are present) anaemia should be suspected, even in the absence of target cells.
Implications
- The abnormal appearance of target cells is due to their abnormal shape. Instead of the normal biconcave shape, the space between the target cell’s central membranes has become very thin, to the extent that they collapse on themselves. They have more membrane material than normal, or a reduced haemoglobin content. They have too much membrane for the amount of haemoglobin.
- Often associated with iron deficiency anaemia, where both target cells and microcytic hypochromic cells will be observed, due to low haemoglobin content of RBCs.
- May also be observed in liver disease, where the cell’s cholesterol to serum phospholipid ratio is increased, due to decreased enzymatic activity of lecithin cholesterol acyltransferase (LCAT).
- May also occur in: haemochromatosis, thalassemia, post splenectomy, dehydration, biliary obstruction, anaemia caused by chronic blood loss (such as found in a bleeding gastric ulcer, Crohn’s disease and haematuria).
Associated Symptoms
- Lassitude
- Dizziness
- Weakness
- Poor concentration
- Pallor
- Shortness of breath
- Increased heart rate
- Palpitations
Interventions
Any combination of the following, depending on the rest of the case:
LIVER PROTOCOL (where target cells are related to a liver condition):
- Avoid alcohol, caffeine, tobacco, saturated/animal fat, sugar, drugs and non-essential medication.
- Hepaton : 30 drops tincture 3x daily. May be increased to 5ml tincture 3xdaily.
SUPPLEMENTS:
- Chelated Iron supplement (when target cells observed & iron deficiency confirmed)
- Trace minerals: Bio-lonic Minerals
Working with
Iron deficiency anaemia is suspected when both target cells and microcytic hypochromic cells are observed. However, in cases where anaemia symptoms are present and more than 10% of the RBCs are microcytic and hypochromic, anaemia should be suspected even in the absence of target cells. Thalassaemia is likely when hypochromic RBCs, target cells and RBCs resembling bowling pins are observed. In cases with target cells and diffuse fibrin in the plasma, a liver condition is the most likely cause. As with most blood morphologies, correlate data to determine the appropriate corrective approach. Beware of haemochromatosis, and always correlate clinically as clients with iron overload may also present with target cells.
General Guidelines
- Moderate, or exclude, animal protein intake, aiming for balanced portions appropriate to body size and activity level
-
Avoid heavy or complex meal combinations; eat slowly, seated, and chew thoroughly to support digestive efficiency
-
Where relevant, consider individualised nutritional approaches that recognise biochemical uniqueness
-
Be mindful of potential food sensitivities or intolerances that may influence systemic balance
-
Increase water intake → Weight (kg) ÷ 8 × 0.25 = litres/day (2-3 litres is the average)
-
Emphasise fibre-rich carbohydrates, leafy greens, sprouts, raw or lightly processed vegetables, and antioxidant-rich whole foods
-
Reduce reliance on highly processed foods, refined carbohydrates, and excessive saturated fats
-
Minimise or avoid smoking, alcohol, excess caffeine, refined sugar, and unnecessary chemical exposure where possible
Functional Systems Influenced
Hematological
Target cells reflect an altered balance between red blood cell membrane surface area and internal content. This directly affects red blood cell structure and how cells behave within the circulating blood.
Hepatic (Liver)
The liver plays a central role in managing fats, proteins, and overall blood composition. Changes in how these components are processed can influence red blood cell membrane characteristics, contributing to the target-like appearance.
Digestive & Nutrient Assimilation
Red blood cell structure depends on the availability and proper handling of nutrients involved in cell formation and membrane maintenance. When digestion or nutrient assimilation is less efficient, red blood cell morphology may reflect these influences over time.
Metabolic
Metabolic processes support red blood cell renewal, turnover, and balance between cell content and membrane structure. Reduced metabolic efficiency can allow altered red blood cell forms to persist in circulation.
Commonly Associated Terrain Imbalances
B12 / Folate insufficiency
These nutrients support red blood cell development and internal structure. Reduced availability may influence how red blood cells distribute their internal contents, contributing to the target-like appearance.
Hepatic overload
The liver plays a central role in managing fats and proteins within the blood. When processing capacity is strained, red blood cell membrane composition may shift, affecting the balance between membrane surface area and internal content.
Iron insufficiency
Iron availability influences red blood cell structure and haemoglobin distribution. Changes in iron handling or utilisation may be reflected in altered internal density patterns within the cell.
Malabsorption / enzyme deficiency
When digestion or nutrient breakdown is less efficient, the components required for balanced red blood cell formation may be inconsistently available, contributing to structural variation.
Omega-3 fatty acids low
Essential fatty acids support healthy, flexible cell membranes. Reduced availability may affect membrane composition, influencing the characteristic ringed appearance of target cells.
Protein intake / albumin low
Adequate protein availability helps maintain balanced plasma and red blood cell structure. Reduced levels may influence the relationship between membrane surface area and internal cell content.
Supportive Focus & Awareness
-
Awareness of factors that support balanced red blood cell membrane structure and internal composition
-
Awareness of liver function as it relates to processing fats and proteins that influence blood composition
-
Awareness of digestive efficiency and how well nutrients are absorbed over time
-
Awareness of long-term nutrient availability that supports healthy red blood cell formation
Commonly Reported Experiences
- Some individuals whose blood patterns include target cells report general feelings of tiredness or low energy, sometimes described as lassitude or weakness. Others may notice difficulty maintaining focus or concentration, particularly during periods of physical or mental demand.
- Light-headedness or dizziness is also sometimes reported, along with a pale or washed-out appearance. In some cases, individuals describe sensations related to circulation or exertion, such as becoming short of breath more easily than expected.
- Awareness of heart activity, including a faster heartbeat or occasional palpitations, is also sometimes mentioned. These experiences are non-specific and can be influenced by many factors, including hydration, activity levels, stress, and overall health.
Their presence does not confirm any condition and should always be considered in the broader context of individual circumstances and other observations.
Systems / Body Functions
Digestive & Nutrient Assimilation, Hematological, Hepatic (Liver), Metabolic
Imbalances
B12 / Folate insufficiency, Hepatic overload, Iron insufficiency, Malabsorption / enzyme deficiency, Omega-3 fatty acids low, Protein intake/albumin low
Target cells are red blood cells that display a distinctive bull’s-eye or target-like appearance, with a darker central area surrounded by a lighter ring and an outer rim. This pattern reflects an altered balance between the red blood cell’s internal content and its surrounding membrane.
In live blood analysis, it is not unusual to observe an occasional target-shaped red blood cell within a field of view. However, when a noticeable proportion of red blood cells show this characteristic appearance across multiple fields, it suggests a broader pattern rather than an isolated variation.
The presence of target cells indicates that red blood cell structure is being influenced by changes in membrane composition or internal distribution, highlighting a blood terrain where balance between cell content and surface area may be altered.
Target cells are erythrocytes that have become parasitised by the endobiont (Mucor racemosus Fresen). Dysbiosis is to be suspected whenever the shape or size of a blood form is disturbed. Codocytes are often observed along with “flimmering” (an acronym for flickering and glimmering, where the central area of the RBC seems to flicker or glimmer) in the RBCs, which indicates parasitism of the RBCs by microorganisms. This is a vegetative process where high-valence symprotits and ascits use a contained environment which provides nutritional reserves for their upward development. This infestation will become obvious in darkfield by pressing lightly on the cover slip with a pointed object like the tip of a pen, which will break up the RBCs and release the colloids from the cells. The advanced phases of the endobiont will often be found to be related to this appearance.
 Disclaimer
Disclaimer