You must be logged in to record observations.
Short Description
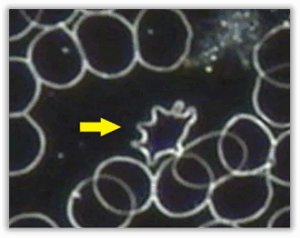
- Acanthocytes are red blood cells that display irregular, unevenly spaced projections extending from the cell surface, giving them a spiky or thorn-like appearance. Unlike cells with uniform surface changes, the projections on acanthocytes vary in length and distribution, resulting in a distinctly distorted outline.
- In live blood analysis, acanthocytes are not typically seen in healthy samples. When they are present, they often stand out clearly due to their pronounced and irregular shape. Observation across multiple fields of view increases the significance of this finding, suggesting a broader influence on red blood cell membrane structure.
- The presence of acanthocytes reflects a change in red blood cell membrane composition and stability, highlighting a blood environment where membrane resilience and balance may be compromised rather than temporarily altered.
Appearance
- The prefix ‘acantha’ in Greek means ‘thorn’. Acanthocytes are abnormally shaped RBCs that have three to ten pronounced, irregular and blunt finger-like projections of varying length and width. They should be distinguished from echinocytes, which have multiple (>10) small, sharp, evenly distributed and regularly shaped spines. Acanthocytes should also be distinguished from poikilocytes, which have rounded, shorter ‘bumps’ at the edge of the RBC membrane, somewhat resembling a bottle cap.
Pleomorphic Perspective
The pathogenesis of acanthocytes in pleomorphism is the same as with the RBCs with single membrane protrusions. Both these forms develop as a result of the bacterial phase of the endobiont’s life cycle. Bacterial rods can be seen emerging from RBCs. These are ascits of Leptotrichia buccalis, the bacterial phase of Mucor racemosus Fresen. They are associated with lowered or deficient resistance. In the case of acanthocytes, when many ascits can be seen emerging from the RBC, it is indicative of a strong endobiontic burden.
Medical Perspective
- The formation of acanthocytes is a consequence of a defect on the erythrocyte cell membrane. Projections from the cell membrane are irregular and distorted, with the apex of the projections being pointed. This distorted shape results from an alteration of the lipid composition and fluidity of the erythrocyte membrane, caused by incorrectly synthesised beta-lipoprotein by the liver and a decreased replacement rate of the membrane cholesterol.
- Acanthocytosis is a red cell phenotype found in various underlying conditions. Abetalipoproteinaemia (Bassen–Kornzweig syndrome) and spur cell haemolytic anaemia of severe liver disease are the most frequent and most significant underlying conditions associated with acanthocytosis. Acanthocytes also occur in neuroacanthocytosis, anorexia nervosa and other malnutrition states, infantile pyknocytosis, McLeod syndrome, Lu null Lutheran phenotype, hypothyroidism, idiopathic neonatal hepatitis and myxoedema. They are also observed with transient haemolysis and stomatocytosis in individuals with alcoholism and mild haemolysis and spherocytosis in individuals with congestive splenomegaly.
- Other conditions associated with acanthocytes include homozygous familial hypobetalipoproteinaemia, Zieve syndrome and chronic granulomatous disease (CGD) associated with McLeod red cell phenotype.
Relevance
- Acanthocytes are not usually observed in normal live blood samples. This finding is significant when seen during analysis, especially if observed in more than 3% of the total RBC sample.
Implications
- Since the liver and spleen contribute to the maintenance of the RBC membranes, the presence of acanthocytes suggest liver and spleen dysfunction.
- This abnormality of the RBC membrane is caused by a change in the lipid distribution in the RBC membrane, resulting in an altered membrane lipid composition. Acanthocytes have excess cholesterol in the cell membrane, which expands the outer leaflet of the lipid bilayer, resulting in blunt, irregular projections.
- Essential Fatty Acid deficiency; Vitamin E deficiency
- Kidney Stress & Potassium loss (ask about diuretic prescription drugs and look for echinocytes).
- Potentially serious liver disease, such as Cirrhosis & Hepatitis)
- High Cholesterol
- Splenic dysfunction, Post-Splenectomy (surgical removal of the spleen). Acanthocytes are observed in these cases because macrophages (WBCs) in the spleen would normally remove these cells from the circulation.
- Anorexia Nervosa
- Cystic Fibrosis
- Myelodysplasia
- Hypothyroidism
Associated Symptoms
- Fatigue
- Drowsiness
- Poor circulation
- Possible signs of liver disease
- Asymptomatic in many cases
Interventions
Any combination of the following, depending on the rest of the case:
KIDNEY PROTOCOL:
- Potassium supplement if kidney stress is suspected (correlate clinically).
- Nephrocil: 30 drops tincture 3x daily. May be increased to 5ml tincture 3xdaily.
- Reduce animal protein and acid-forming foods.
SUPPLEMENTS:
- Omega-3 supplement (1000-2000 EPA daily).
- Vitamin E: start with 400mg daily and gradually increase to 800mg daily.
- Buffered vitamin C (2500mg).
Working with
- Most cases of mild acanthocytosis respond to nutritional interventions. Focus is placed on correcting dietary fat digestion, essential fatty acid deficiency, vitamin and trace mineral deficiencies, while supporting the liver, kidneys and other organs of elimination. If the condition does not improve further conventional investigations may be necessary (especially in cases with marked acanthocytosis).
General Guidelines
General Guidelines:
- Increase water intake: Weight (kg) ÷ 8 × 0.25 = litres/day.
- Increase intake of fibre-rich carbohydrates and raw, polyunsaturated fats.
- Avoid saturated fat, refined carbohydrates and enzyme-deficient foods.
- Avoid alcohol, caffeine, sugar, drugs and non-essential medication.
- Include raw vegetable juices, sprouts, greens and superfoods.
- Increase essential minerals and electrolyte intake
- Test and treat high cholesterol if present.
- Treat hypothyroidism if present.
- Thyroid Formula
Functional Systems Influenced
Hematological
Acanthocytes indicate that some red blood cells have lost their usual smooth, flexible shape. This matters because red blood cells need to remain adaptable in order to move easily through small blood vessels and deliver oxygen efficiently. When their shape becomes irregular, circulation at the micro level may be less efficient, which can influence overall energy, stamina, and tissue support.
Hepatic (Liver)
The liver plays a central role in managing fats, proteins, and other substances that contribute to healthy red blood cell membranes. When liver processing is under strain, red blood cell structure may reflect this through altered surface patterns. This does not point to a diagnosis, but rather suggests that the body’s internal processing and balance systems may benefit from additional support or attention.
Oxidative & Antioxidant Balance
Red blood cell membranes are particularly sensitive to oxidative stress. When antioxidant protection is reduced, cell surfaces can become less stable and more irregular over time. This may affect how resilient red blood cells are as they circulate, especially under physical or metabolic demands, highlighting the importance of maintaining adequate antioxidant balance.
Commonly Associated Terrain Imbalances
Hepatic overload
Acanthocytes are closely linked to altered lipid handling, and the liver plays a central role in regulating fats and membrane components. When hepatic processing is under strain, red blood cell membranes may lose uniformity and develop irregular projections.
Sluggish bile / detox pathways
Efficient bile flow is essential for fat metabolism and clearance. When this process slows, membrane composition can be affected, reducing flexibility and contributing to distorted red blood cell surfaces.
Omega-3 fatty acids low
Omega-3 fats are critical for maintaining flexible, resilient cell membranes. Reduced availability can lead to stiffer membranes that are more prone to irregular surface formations such as acanthocytes.
Oxidative stress
Ongoing oxidative pressure can damage or weaken red blood cell membranes over time. This reduces structural resilience and increases the likelihood of irregular, spiculated cell shapes.
Low antioxidant reserve
When antioxidant protection is limited, red blood cells are less able to defend their membranes against daily oxidative challenges, allowing structural distortion to persist.
Supportive Focus & Awareness
- Awareness of factors that support healthy red blood cell membrane structure and resilience
-
Awareness of hydration and fluid balance as they relate to circulation quality
-
Awareness of oxidative balance and everyday influences on cellular stability
-
Awareness of digestive efficiency and long-term nutrient availability
-
Awareness of energy levels, stamina, and recovery under physical or metabolic demand
Commonly Reported Experiences
- Some individuals with blood patterns that include acanthocytes report experiences such as reduced stamina, feeling fatigued more easily under physical or mental demand, or slower recovery after exertion. Others may notice sensations related to circulation, such as feeling colder in the hands or feet.
These experiences are non-specific and can be influenced by many factors. Their presence does not confirm any condition but may provide helpful context when considered alongside other observations and personal circumstances.
Systems / Body Functions
Hematological, Hepatic (Liver), Oxidative & Antioxidant Balance
Imbalances
Acidic terrain, Hepatic overload, Low antioxidant reserve, Malabsorption / enzyme deficiency, Omega-3 fatty acids low, Protein intake/albumin low
- Acanthocytes are red blood cells that display irregular, unevenly spaced projections extending from the cell surface, giving them a spiky or thorn-like appearance. Unlike cells with uniform surface changes, the projections on acanthocytes vary in length and distribution, resulting in a distinctly distorted outline.
- In live blood analysis, acanthocytes are not typically seen in healthy samples. When they are present, they often stand out clearly due to their pronounced and irregular shape. Observation across multiple fields of view increases the significance of this finding, suggesting a broader influence on red blood cell membrane structure.
- The presence of acanthocytes reflects a change in red blood cell membrane composition and stability, highlighting a blood environment where membrane resilience and balance may be compromised rather than temporarily altered.
The pathogenesis of acanthocytes in pleomorphism is the same as with the RBCs with single membrane protrusions. Both these forms develop as a result of the bacterial phase of the endobiont’s life cycle. Bacterial rods can be seen emerging from RBCs. These are ascits of Leptotrichia buccalis, the bacterial phase of Mucor racemosus Fresen. They are associated with lowered or deficient resistance. In the case of acanthocytes, when many ascits can be seen emerging from the RBC, it is indicative of a strong endobiontic burden.
 Disclaimer
Disclaimer