Appearance
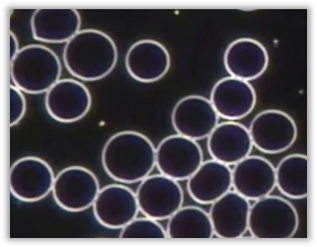
The majority of RBCs vary greatly in shape and size, displaying irregular edges, varying sizes, membrane projections and fragments. Some RBCs are rod-shaped or may resemble bowling pins. Target cells are usually also present.
Relevance
In normal live samples all the RBCs should generally be the same size and circular in shape.
Implications
- Possible thalassaemia
- Iron deficiency anaemia
- Haemolytic anaemia
Associated Symptoms
• May be asymptomatic
• Lassitude
• Dizziness
• Weakness
• Poor concentration
• Pallor
• Shortness of breath
• Increased heart rate
• Palpitations
Pleomorphic Perspective
This anomaly is caused by a pathogenic influence of the endobiont on the erythrocytes. Careful inspection will reveal that there are advanced phases of the endobiont occurring. This infestation will become obvious in darkfield by pressing lightly on the cover slip with a pointed object like the tip of a pen, which will break up the RBCs and release the chondrits from the cells.
Medical Perspective
Anisopoikilocytosis may be observed in peripheral blood smears of patients with iron deficiency and/or thalassaemia.
Interventions
Any combination of the following, depending on the rest of the case:
SUPPLEMENTS:
- Chelated Iron supplement
- Trace minerals: Bio-Ionic Mineral Concentrate (Neogenesis Health Products)
GENERAL GUIDELINES:
- Increase water intake. To determine necessary daily water intake (in litres): Weight (kg) / 8 × 0.25
- Increase chlorophyll-rich foods: chlorella, spirulina, wheatgrass juice/powder, barley grass juice/powder, alfalfa tablets, green leafy vegetables
- Blackstrap molasses
- Avoid saturated fat, refined carbohydrates and food deficient in natural enzymes. • Avoid alcohol, caffeine, sugar, drugs and non-essential medication
- Raw vegetable juices (greens & beet), sprouts and superfoods.
- Test for Thalassaemia (FBC, Iron studies & Haemoglobin Electrophoresis).
Working with Anisopoikilocytosis
This is usually observed in patients with severe iron deficiency anaemia or thalassaemia. Further testing is recommended in patients with moderate to severe anisopoikilocytosis. Testing includes FBC, Iron studies, Haemoglobin Electrophoresis and investigations to determine the cause of iron deficiency where thalassaemia has been excluded, as this may be due to chronic blood loss (e.g., from a bleeding gastric ulcer). Iron supplementation is indicated in the majority of these cases.
Further Investigations
- FBC + Differential + ESR
- Peripheral blood smear microscopy
- Iron Studies
- Haemoglobin Electrophoresis
- Liver Function Test (LFT)
- Abdominal Ultrasound / Abdominal MRI
- Gastroscopy, Colonoscopy
 Disclaimer
Disclaimer