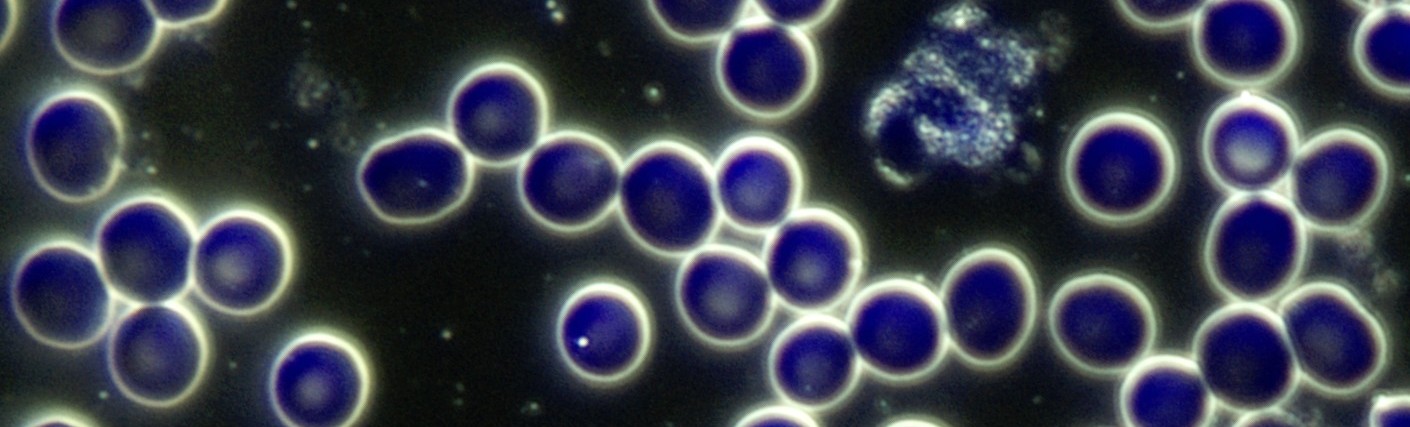
Appearance
The term “target cell” arises from the cell’s resemblance to a target. Also referred to as codocytes and anulocytes, these cells range from hypochromic cells, where the central area of pallor is much larger and more defined than usual, to true target cells that contain a bull’s-eye in the centre of the cell. This appearance is due to the RBC’s abnormal shape.
Relevance
Target cells can be present in the blood of healthy individuals, but usually comprise less than 1% of the RBC population. The presence of more than 5 target cells in a sample would be considered a significant finding, especially if accompanied by anaemia symptoms. However, if more than 10% of the RBCs are microcytic and hypochromic (and anaemia symptoms are present), anaemia should be suspected even in the absence of target cells.
Implications
- The abnormal appearance of target cells is due to their abnormal shape. Instead of the normal biconcave shape, the space between the target cell’s central membranes becomes very thin, causing them to collapse on themselves
- They may have more membrane material than normal or reduced haemoglobin content — too much membrane for the amount of haemoglobin
- Often associated with iron deficiency anaemia, where both target cells and microcytic hypochromic cells are observed, due to low haemoglobin content.
- May also be observed in liver disease, where the cell’s cholesterol to serum phospholipid ratio is increased due to decreased enzymatic activity of lecithin cholesterol acyltransferase (LCAT)
- May also occur in haemochromatosis, thalassaemia, post-splenectomy, dehydration, biliary obstruction, anaemia caused by chronic blood loss (such as from a bleeding gastric ulcer, Crohn’s disease, or haematuria).
Associated Symptoms
• Lassitude
• Dizziness
• Weakness
• Poor concentration
• Pallor
• Shortness of breath
• Increased heart rate
• Palpitations
Pleomorphic Perspective
Target cells are erythrocytes that have become parasitised by the endobiont (Mucor racemosus Fresen). Dysbiosis is to be suspected whenever the shape or size of a blood form is disturbed. Codocytes are often observed along with “flimmering” (an acronym for flickering and glimmering, where the central area of the RBC seems to flicker or glimmer) in the RBCs, which indicates parasitism of the RBCs by microorganisms. This is a vegetative process where high-valence symprotits and ascits use a contained environment which provides nutritional reserves for their upward development. This infestation will become obvious in darkfield by pressing lightly on the cover slip with a pointed object like the tip of a pen, which will break up the RBCs and release the colloids from the cells. The advanced phases of the endobiont will often be found to be related to this appearance.
Medical Perspective
Hypochromia occurs when an erythrocyte contains a decreased amount of haemoglobin. It appears as a larger-than-normal central area of pallor with a thin rim of haemoglobin. This is one of the most commonly observed types of abnormal erythrocytes, seen in iron-deficiency anaemia and thalassaemia. It may also be seen in any haemoglobinopathy. Codocytes are erythrocytes that exhibit a dark circular ‘target’ pattern. They are seen in hypochromic anaemia, liver disease and occasionally after splenectomy. Erythrocytes with this configuration are cells lacking iron; therefore, any disease process that affects red cell iron absorption may produce target cells. Marked elevations of target cells can also result from a shift in the exchange equilibrium between red cells and cholesterol. Conditions that reduce lecithin-cholesterol acyltransferase production or interfere with enzyme mechanisms of performance result in elevated red cell cholesterol and serum phospholipid ratios. The bile salts content ratio in plasma can also affect cholesterol exchange between plasma and red cell membranes.
Interventions
Any combination of the following, depending on the rest of the case:
LIVER PROTOCOL (where target cells are related to a liver condition):
- Avoid alcohol, caffeine, tobacco, saturated/animal fat, sugar, drugs, and non-essential medication.
- Hepaton (Neogenesis Health Products): 30 drops tincture 3× daily. May be increased to 5ml tincture 3× daily
SUPPLEMENTS:
- Chelated Iron supplement (when target cells observed and iron deficiency confirmed)
- Trace minerals: Bio-Ionic Mineral Concentrate (Neogenesis Health Products)
GENERAL GUIDELINES:
- Increase water intake. To determine necessary daily water intake (in litres): Weight (kg) / 8 × 0.25
- Increase chlorophyll-rich foods: chlorella, spirulina, wheatgrass juice/powder, barley grass juice/powder, alfalfa tablets, green leafy vegetables.
- Blackstrap molasses.
- Avoid saturated fat, refined carbohydrates and food deficient in natural enzymes
- Avoid alcohol, caffeine, sugar, drugs and non-essential medication.
- Raw vegetable juices (greens & beet), sprouts and superfoods.
Working with Target Cells
Iron deficiency anaemia is suspected when both target cells and microcytic hypochromic cells are observed. However, in cases where anaemia symptoms are present and more than 10% of the RBCs are microcytic and hypochromic, anaemia should be suspected even in the absence of target cells. Thalassaemia is likely when hypochromic RBCs, target cells and RBCs resembling bowling pins are observed. In cases with target cells and diffuse fibrin in the plasma, a liver condition is the most likely cause. As with most blood morphologies, correlate data to determine the appropriate corrective approach. Beware of haemochromatosis, and always correlate clinically as clients with iron overload may also present with target cells.
 Disclaimer
Disclaimer